INTRODUCTION:
Production of erythrocytes in
the marrow occurs at the staggering rate of more than 2 million cells
per second. For this production to occur, a number of raw materials
must be present in adequate amounts. These include the same nutrients
that are essential to the production and maintenance of any cell,
such as glucose, lipids, and amino acids. However, erythrocyte
production also requires several trace elements:
2)
Copper: A trace mineral,
copper is a component of two plasma proteins, hephaestin and
ceruloplasmin. Without these, hemoglobin could not be adequately
produced. Located in intestinal villi, hephaestin enables iron to be
absorbed by intestinal cells. Ceruloplasmin transports copper. Both
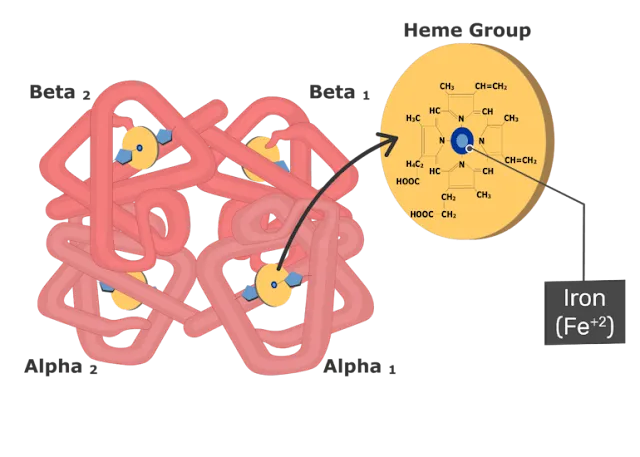
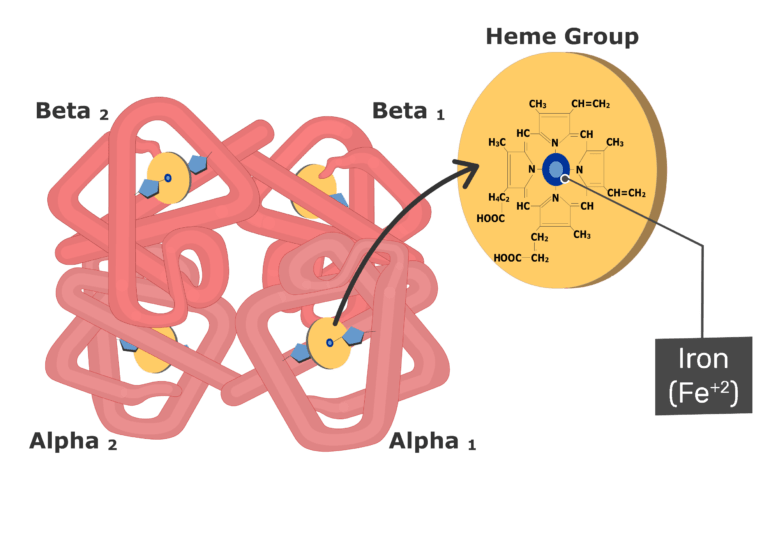
enable the oxidation of iron from Fe2+
to Fe3+,
a form in which it can be bound to its transport protein,
transferrin, for transport to body cells. In a state of copper
deficiency, the transport of iron for heme synthesis decreases, and
iron can accumulate in tissues, where it can eventually lead to organ
damage.
3)
Zinc: The trace mineral zinc
functions as a co-enzyme that facilitates the synthesis of the heme
portion of hemoglobin.

In the large intestine,
bacteria breaks the bilirubin apart from the bile and converts it to
urobilinogen and then into stercobilin. It is then eliminated from
the body in the feces. Broad-spectrum antibiotics typically eliminate
these bacteria as well and may alter the color of feces. The kidneys
also remove any circulating bilirubin and other related metabolic
byproducts such as urobilins and secrete them into the urine.
The breakdown pigments formed from the destruction of hemoglobin can
be seen in a variety of situations. At the site of
an injury, biliverdin from damaged RBCs produces some of the dramatic
colors associated with bruising. With a failing liver, bilirubin
cannot be removed effectively from circulation and causes the body to
assume a yellowish tinge associated with jaundice. Stercobilins
within the feces produce the typical brown color associated with this
waste. And the yellow of urine is associated with the urobilins.
RELATED;
1.
THE HUMAN RED BLOOD CELLS
2.
HEMOGLOBIN THE OXYGEN TRANSPORTER
3.
BLOOD AND IT’S COMPONENTS
REFERENCES













No comments:
Post a Comment